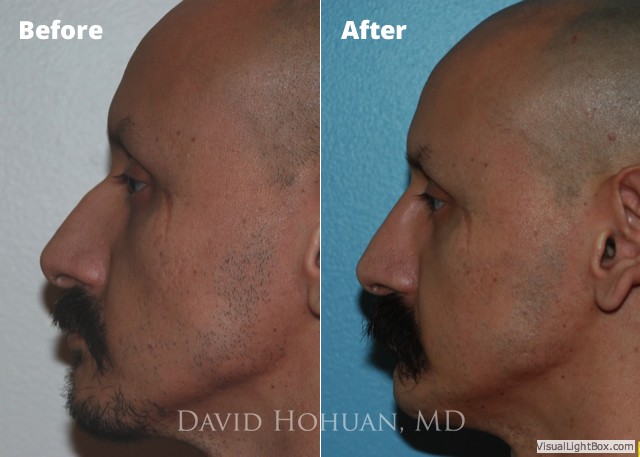
Rhinoplasty, also referred to as a ‘nose job,’ involves making structural changes to the nose to create a more desirable contour and shape. Rhinoplasty has remained a very popular procedure, due to its ability to make dramatic changes in one’s facial appearance. Dr. Hohuan understands this can have a very positive impact on one’s self-esteem.
Rhinoplasty is considered by most surgeons to be the most complex of all plastic surgeries of the face, and careful selection of a Rhinoplasty surgeon is essential. To obtain consistently good results, the facial plastic surgeon must be skilled in all types of noses and be proficient in advanced techniques. Without the appropriate training and experience, obtaining these results becomes more of a random process.
During your consultation, all aspects of your nose will be carefully examined, and photographs will be taken in different views. You will meticulously review these photos with Dr. Hohuan while he ascertains your goals and wishes in terms of any changes in form and function that are desired. This may be done in conjunction with a photo simulation tool. Dr. Hohuan will explain how best to achieve the desired goals, whether through an open or closed approach. Most changes to the nasal sidewall and dorsum or bridge can be done with small access incisions through the inside of your nose (closed or endonasal rhinoplasty). If refinement of the nasal tip is desired, this will usually require a small incision between the nostrils (open rhinoplasty) to allow the most precise positioning of nasal tip cartilage. If you have had previous nasal surgery, Dr. Hohuan will discuss any additional procedures that are required to obtain the desired improvement in form and function (ear cartilage grafts, rib cartilage grafts, temporalis fascia grafts).
Dr. Hohuan believes that rhinoplasty is the most challenging procedure performed in facial plastic and reconstructive surgery. However, it is also perhaps the most rewarding for both patient and surgeon. Dr. Hohuan has trained with some of the finest head and neck surgeons and plastic surgeons in the world. Dr. Hohuan has made it his goal to master this complex operation and follow in the footsteps of the rhinoplasty pioneers who trained him.





Within the field of plastic surgery, rhinoplasty is without a doubt one of the most challenging procedures to perform. There are many reasons for this. Principal among them is achieving a high degree of control over how cartilage, bone, and a patient’s soft-tissue-skin-envelope heal over time. Things may be adequate for the first year or two. However, unless your surgeon employed techniques that can resist scar contracture, over time the shape of someone’s nose may undergo significant unwanted changes.
Another reason is that the changes we are trying to achieve in rhinoplasty is often on the order of millimeters. Therefore, the execution of surgical techniques is paramount, and your surgeon must have the training, judgement, and patience intraoperatively to get you the result that is going to last you your lifetime. It is hard to dabble in rhinoplasty surgery. My advice is to find a surgeon who is passionate about rhinoplasty, who performs these on a regular basis, and who has advanced training in rhinoplasty. I am a double-board certified facial plastic surgeon who has performed several hundreds of rhinoplasties. Unlike some other plastic surgeries, rhinoplasty takes a certain amount of regular dedication and practice to deliver consistent, natural, and beautiful results.
The most challenging rhinoplasties to perform are revision rhinoplasties. At the same time, they are often the most rewarding. I have seen and treated many patients from throughout California, Arizona, and Mexico who have had previous rhinoplasties that for one reason or another, did not turn out satisfactory for the patient. Poor results in rhinoplasty can be absolutely devastating for the patient. It takes an incredible amount of planning to achieve correction. Often, patients may lack cartilage in their nose from their previous surgery. This requires additional grafts in the form of ear cartilage, rib cartilage, or soft tissue from behind the hairline (temporalis fascia) to correct the deformity. The challenge with these cases is the unpredictability of what previous surgeons may have done in the nose. Intraoperatively, you must be able to improvise and have multiple ways of repairing something unwanted. Because of how much purely reconstructive rhinoplasty I have done for patients who have sustained trauma to the face from gunshots, motor vehicle accidents, and cancer resections, I can apply these techniques if the situation calls for it.
These terms specify different surgical approaches and techniques to rhinoplasty. Closed rhinoplasty does not utilize any incisions on the skin. Open rhinoplasty is performed with a small incision between a patient’s nostrils that if executed correctly, should heal imperceptibly. Ideally, your surgeon should be versatile and facile in both techniques. Once you have mastered both approaches, you can become more efficient with your surgery. I have spent my professional life striving for mastery of both approaches. Therefore, depending on the specific changes that a patient would like, different techniques are more suited. For example, there is no need for an open approach if you are principally changing the profile of a nose. Alternatively, if you are making significant changes to the tip, an open approach provides the maximum amount of precision and placement of grafts. After your full facial consultation with me, we will discuss and analyze your photos and determine what your main goals are. The surgical approach depends on that.
I do not use packing after rhinoplasty, whether cosmetic or solely for relief of nasal obstruction. I do use plastic splints that are about the thickness of a leaf of paper, and are gently placed in the nose and removed after 5-6 days. Most patients are minimally bothered by this, but there can be slight discomfort when these small splints are removed. The discomfort is mild to moderate and lasts a few seconds. It is never more than moderate.
There is usually minimal to no bruising underneath the eyes unless you underwent osteotomies. This is something I usually discuss with patients during the comprehensive facial and nasal consultation. Osteotomies are usually necessary when we are trying to make changes to the width of the base of the upper 1/3 of the nose, if we are trying to change the slope or slant of the nasal bones, or if we are doing a major reduction in the profile.
This depends on the extent of surgery. Generally, patients undergoing “open” rhinoplasty have more swelling than patients undergoing “closed” rhinoplasty.” Most of the swelling in the upper 1/3 of the nose along the bones is gone at the end of 3 months. Most of the swelling in the middle 1/3 of the nose is gone at the end of 6 months. Most of the swelling in the tip is gone at 9 months. That is why we do not consider revision rhinoplasty until at least 9-12 months after the first surgery because the nose remodels. The swelling I have referenced above is subtle however, and can be noticed with close inspection, usually by the patient, surgeon, and very close family and social contacts. To the casual observer, a patient is presentable at 2-3 weeks with make-up. At 2 months, a casual observer may fail to notice any swelling. The patients who have the least swelling are those undergoing closed rhinoplasty for minor changes to the profile. The patients who have the most swelling are those undergoing major revision rhinoplasty with rib cartilage.
Everybody is different. Most of my patients have mild to moderate pain rhinoplasty. It is rare for patients to experience severe pain. Most of the pain is very manageable with narcotic medications such as Vicodin or Percocet.
The inability to breathe through the nose with the need for mouth-breathing seems to be the thing patients complain about most. We help alleviate this by having patients rinse their nose with saline frequently throughout the first 6 weeks after surgery. By the time patients are seen for their 5-6 day post-operative visit for removal of splints, there is significant relief in this post-operative symptom. However, it takes a full 6 weeks for most of the swelling within the lining of the nose to go down where the final result of breathing can be assessed.
All of my patients receive detailed instructions on their do’s and don’ts. There are separate instructions for those undergoing “closed” vs “open” rhinoplasty. In a nutshell, cool compresses are used around the nose and eyes for the first 48 hours or 2 days after surgery, followed by warm compresses starting on the third day. We have patients do this for 10 minutes every 1 hour while awake. Additionally, we ask that patients restrict alcohol intake for one week before and after surgery, to refrain from aerobic activity for 2 weeks after surgery other than light impact, and to use nasal saline rinses or sprays frequently throughout the day for the first 6 weeks after surgery.
I usually permit patients to return to work or school once their nasal cast and nasal splints are removed after the 5th or 6th day after surgery. As long as they are not taking any narcotic medication which can impact judgement or memory, there is no restriction on any cognitive work. However, patients must abstain from any moderate or rigorous physical activity for a full 14 days after surgery. Increasing your heart rate significantly can cause significant swelling to the face, leading to prolonged recovery, bleeding, and issues with wound healing.
There are many things I enjoy about rhinoplasty. It is for me personally the most enjoyable operation because it requires an elevated level of planning, judgement, foresight, and skill. Every rhinoplasty operation is extremely individualized and unique, so every time it is performed it is new and different.